The New England Journal of Medicine had a recent article titled, “Physicians, Corporatization, and the Unmeasured Quality of Care.” written by Lawrence Casalino (Division of Health Policy and Economics in the Department of Population Health Sciences at Weill Cornell Medicine, New York). The article, unfortunately, is behind a paywall. Perhaps your local library has a free link.
I love this article for many reasons. The basic premise is that financial measurement of compassionate patient care should be considered in United States healthcare. If you can’t measure it, you can’t reimburse it accurately. This issue leads to the bigger problem of the ethics of “paying” for compassion in medicine.
Let me give you an example. Replacing a knee in an older person is a very complex and important orthopedic procedure. After becoming proficient, this procedure for an orthopedic surgeon understandably becomes rote in how the procedure works. A typical knee replacement takes 90 minutes and reimburses an average of $30,000 with a cost range of $15,000 – $50,000.
Let me give you another example. A pediatrician in the clinic setting has a child come in with malnutrition and who also has experienced potential child abuse. This issue takes a LONG time…examination, labs, talking to the hospital about potential hospitalization, finding a dietician that works with the family’s insurance (or lack of), finding appropriate social services, and even calling the police department. Keep in mind that it is hard to find reimbursement costs for pediatric care because children aren’t covered by Medicare. However, this 90 minute – 120 minute visit which takes significant mental concentration will reimburse anywhere between $150 to $350.
Both the orthopedic surgeon and the pediatrician can be extremely caring people and probably are wonderful. However, should their reimbursement be the same? Should it stay so different? No one really knows. I have strong opinions here, but I could be quite wrong.

This is one of the points of the article. Mainly, can we actually pay for altruistic care?
A quote from the article: “In a classic article, Nobel Prize–winning economist Kenneth Arrow argued that physician ‘behavior is supposed to be governed by a concern for the customer’s welfare which would not be expected of a salesman.'” By the way, here is the open access article originally written by Arrow.
Casalino also states, “My colleagues and I recently used a well-established type of economic experiment to measure altruism, assessing the extent to which people shared money available in the experiment with an unidentified person. We found that although only one third of physicians acted highly altruistically, the average physician acted more altruistically than members of the general population and much more altruistically than the average highly educated, high-income person. We also found evidence that patients of physicians categorized as altruistic had fewer potentially preventable emergency department visits and fewer potentially preventable hospital admissions than patients of other physicians.”
I was interested here and pulled up the study that Casalino and others performed. Thankfully, this article also is open access.

What do we make of all of this? Let me put down some thoughts.
- Physicians who are altruistic probably are safer. Of course, there are so many variables here. A very altruistic neurosurgeon still will have complications because she often takes care of the sickest patients in the hospital. This aspect is NOT her fault. The problem arises with inherent patient pathology.
- Current medical care in the United States does not pay for altruism. It pays for patient volume and pays for procedures. I am a pediatric gastroenterologist. This problem is quite true in my field. I am not saying necessarily that universal / nationalized health systems are better. These systems have their own issues with outcomes, patient wait times, and intractable problems with emergency services. However, universal healthcare is not terrible. As an example, patients with cystic fibrosis in Canada seem to live 10 years longer than patients with cystic fibrosis in the United States. Here is the open access link. Keep in mind that cystic fibrosis care is extremely expensive yet much cheaper in Canada compared to the U.S.
- If we emphasize patient volume and procedure volume in the United States, are we also emphasizing quality care? Not always. Are we emphasizing altruism? Definitely no.
- Late stage capitalism: I pretty much define this term as capitalism that has become so out of control (i.e., too expensive) that eventually the system needs to change. In fact, it is forced to change due to the downstream effects of income inequality, food insecurity, and other related issues. A good review of this terminology from Canada is here. A good review of how late stage capitalism has affected higher education is here. I have no issues with capitalism. I DO have an issue when it gets so out of control that people go bankrupt because of medical debt. I frequently see this tragedy in my medical practice.
- Is human altruism connected to making money? I don’t think so. Is human altruism connected to late stage capitalism? No. They are antithetical to each other.
- Altruism: I think there are two perspectives here. From a genetic perspective, altruism can be defined as caring for others at the expense of one’s survival and/or at the expense of one’s genetics in term of passing one’s genes to further generations. Altruism, as a result, can improve the survival of one’s relatives, one’s species, or one’s society at the expense of the individual. There also is a subjective component here. Humans often demonstrate altruism due to simply caring for or loving the other with no strings attached. It has even been argued that humans can prefer to practice altruism at the expense of our survival. I’m not sure this fact is true. I have no clue.
- However, it may be true if there is a metaphysical aspect here. Suppose we are altruistic because we think or we know God wants us to care for the other. This yearning is not about getting an “award” in the afterlife. This yearning is simply loving the “other” with no strings attached. Suppose we are altruistic because we think or we know that promoting love of the other (family, non-relatives, other types of life, our planet) promotes creativity and promotes love in nature. I think this statement is very true. It seems to be a big part of our religions. Matthew 25: 40 states, “Truly I tell you, whatever you did for one of the least of these brothers and sisters of mine, you did for me.” I’m a Christian, so this verse is important to me. In Islam, Quran 51: 19 states, “And in their wealth there was a rightful share ˹fulfilled˺ for the beggar and the poor.” In Buddhism, Itivuttaka 75 states, “Having rightly amassed wealth attained through initiative, he satisfies rightly with food and drink those fallen into the homeless state.” All of these verses are profound.
- Perhaps our tendency to follow our holy books throughout a significant portion of humanity’s history combined with the genetic aspects of altruism is an epigenetic phenomena.
But consider…just perhaps altruism is humanity’s drive to align with the Divine for love and creativity. For the love of other humans. For the love of all of nature.

Our current healthcare system (at least in the United States) is not built for the love of the other. Late-stage capitalism, no matter how it is defined, does not seem to align with the love of the other. We all have a choice to care for the other, individually or societally, even when market forces work against us.
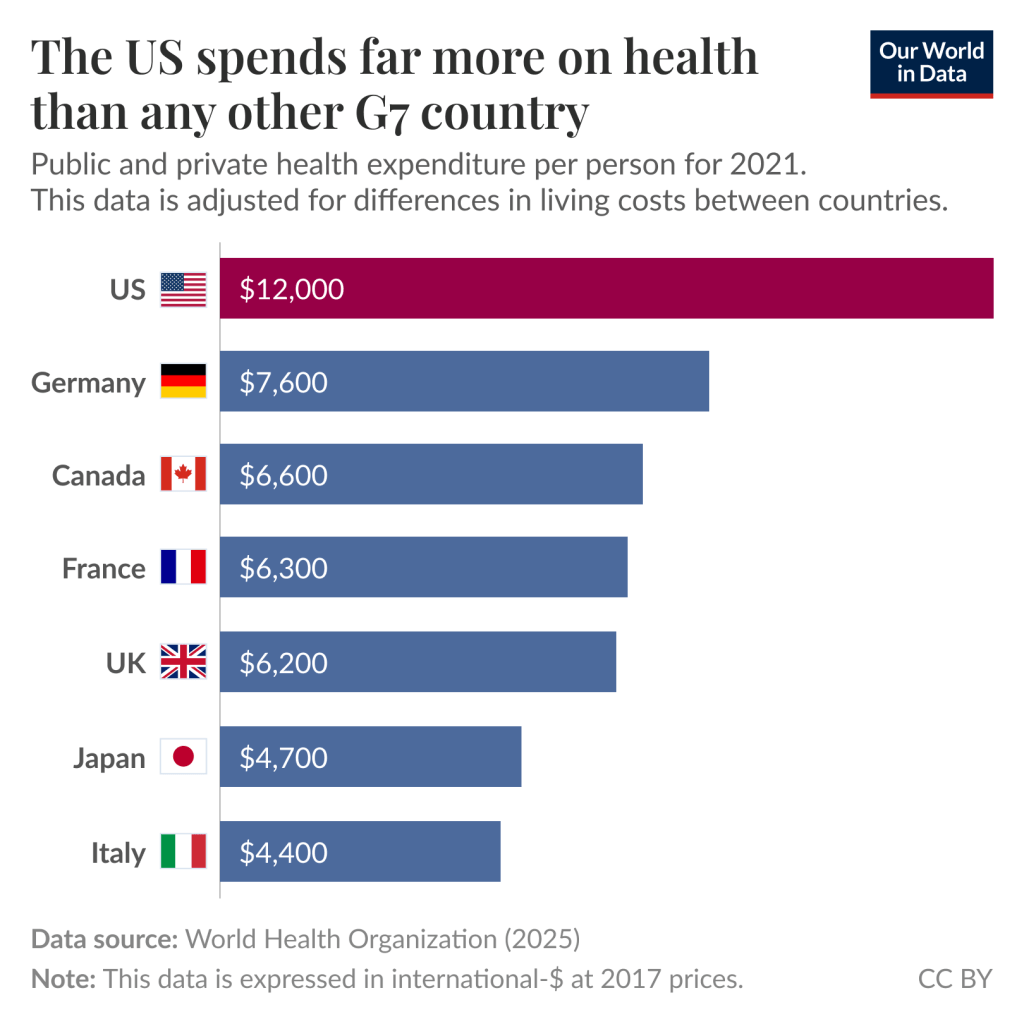
Image from Our World in Data
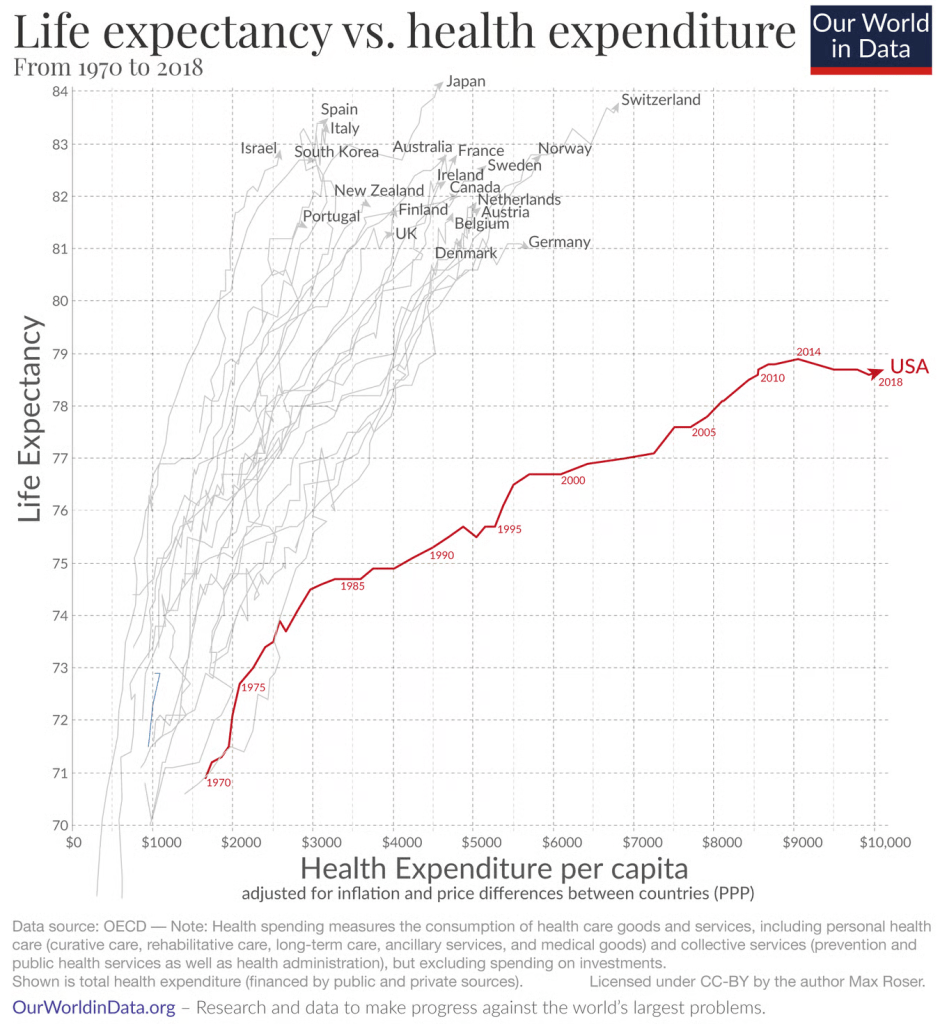
Another image from Our World in Data

Image made by Gemini Advanced
